

ABSTRACT
Sialoliths or salivary gland stones are one of the most common disorders of salivary glands and account for the majority of cases of obstruction within the gland or duct. Their presence may lead to pain, swelling, and discomfort when eating. The submandibular gland is the commonest site of involvement due to its peculiar anatomy. The parotid, sublingual, and minor salivary glands are less commonly involved. This case report highlights the removal of a large Sialoliths from the submandibular gland duct measuring 38mm by 14mm.
Keywords: Sialadenitis; Submandibular Sialolithiasis; Transoral; Anaesthesia; Sialendoscopy
INTRODUCTION
Sialolithiasis is a benign clinical condition characterized by the formation of calcified deposits within the salivary gland system, leading to partial or complete obstruction of salivary flow and resulting in acute or chronic gland inflammation [1,2]. The true prevalence of Sialoliths may be difficult to determine, as many cases may present with no symptoms. However, some studies estimate its prevalence to be about 1.2% of the adult population, with males affected twice as much as females [3]. The condition appears to be rare in children [4]. The formation of salivary stones has been attributed to factors that cause pooling, including anatomical irregularities, local irritants, dehydration, smoking, and the use of certain medications. Salivary gland stones can vary in size from a few millimeters to several centimeters. The submandibular gland accounts for about 80% of salivary stones due to peculiar anatomical factors [5]. Treatment options range from conservative management to more aggressive interventions [6].
CASE REPORT
A 23-year-old male youth corps member was referred to the oral medicine unit of the Randle General Hospital with a chief complaint of painful swelling under the tongue which was associated with an unpleasant taste. His current symptoms had been present for about eight weeks prior to presentation and worsened at meal times. Oral functions such as speech, mastication, and swallowing were preserved. His medical, dental, and social history were uneventful, and he was not on routinely prescribed medications.
Examination showed grossly normal extra-oral features with mild tenderness of the left submandibular region. Mouth opening was adequate with a hard, tender mass noted in the anterior part of the left floor of the mouth. The opening of the left Wharton's duct appeared erythematous with purulent exudate expressed by gentle, firm pressure.
The history and clinical examination were in keeping with a diagnosis of sialadenitis secondary to left submandibular gland Sialolithiasis.

Figure 1: Clinical photograph of left sublingual swelling at presentation
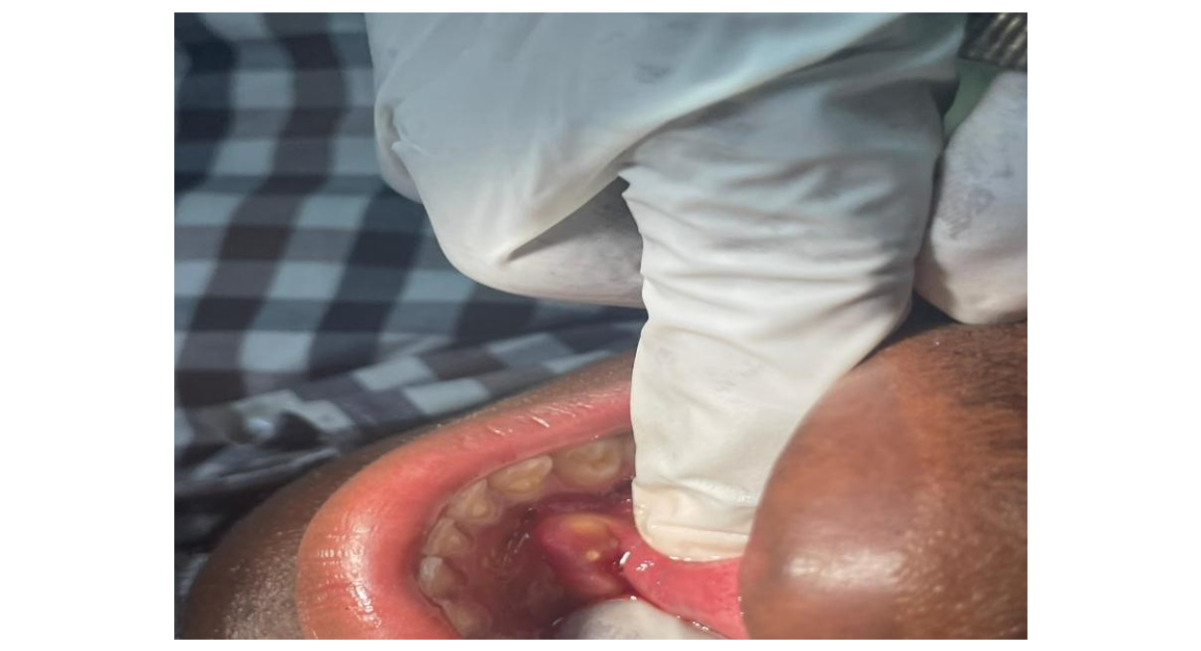
Figure 2: Purulent exudate expressed on firm pressure
Following informed consent, the sialolith was removed via a Transoral approach under local Anaesthesia. An incision was made over the suspected sialolith to expose it, and carefully dissected from the duct. A hard yellowish mass measuring about 38mm by 14mm was retrieved. Postoperative instructions were given, and he was placed on tabs Augmentin 625mg 12 hourly and tabs Metronidazole 400mg 8 hourly for 5 days with tabs diclofenac 50mg b.d for 3 days. A follow-up review was done after 48 hours and showed normal salivary flow and substantial relief of previous symptoms. Another follow-up was done 2 weeks later with no complications noted.

Figure 3: Post-operative clinical photograph after Sialolith removal

Figure 4: Sialolith retrieved from the left submandibular duct

Figure 5: Suture placement after Sialolith removal
DISCUSSION
Sialolithiasis is a salivary gland disorder that can result in the formation of stones within the gland or its duct. Salivary stones can obstruct the flow of saliva and result in gland dysfunction. The prevalence of salivary stones is estimated to be about 1.2 % with a higher occurrence in males and occurring rarely in children [6].
The mechanism of sialolith formation is linked to the deposition of calcium salts around a nidus of organic material such as bacteria, desquamated epithelial cells or mucous. Omokanye described the physiochemical components of a sialolith as predominantly made up of calcium (Ca), sodium (Na), potassium (k), iron (Fe), zinc (Zn), and manganese (Mn) while trace elements include lead (Pb), Cadmium (Cd), Carbon (C), and Silicon (S) [7]. The formation of Sialoliths has been linked to smoking, dehydration, trauma to the gland or duct, and factors leading to salivary stasis [8]. Other factors directly related to the salivary glands include increased alkalinity and calcium content of saliva, inflammation or infection of the salivary duct or gland.
The submandibular gland is the most common site of stone formation due several factors such as a higher alkaline and mucus content, higher concentration of calcium and phosphate, a wider and longer duct compared to other glands, and the flow of saliva against gravity [9,10].
The consequences of a stone within the salivary gland or duct depend on its size, which ultimately determines the degree of obstruction. Smaller stones are often asymptomatic and may be discovered incidentally, while larger stones can lead to pain, swelling, superimposed bacterial infection and compromised gland function that necessitates gland removal [11,12]. Stones measuring above 15mm are rare, and few have been reported in the literature [7].
The management of Sialoliths depends on their size and location, and treatment is generally aimed at restoring salivary flow, preventing infection, and when possible, avoiding gland removal. For small superficial Sialoliths, conservative methods such as gland massage and the use of sialogogues have been adopted [13]. For larger and more deeply positioned stones, extra-corporeal shock wave lithotripsy, Sialendoscopy, or gland removal are treatment options. In this case report, sialolith removal was performed Transorally under local Anaesthesia with preservation of the submandibular gland.
CONCLUSION
The Transoral removal of large Sialoliths from the submandibular gland or duct is a minimally invasive treatment approach in the management of Sialolithiasis. Adequate post-operative follow-up is essential to minimise complications and ensure optimal recovery.
FUNDING
None
CONFLICT OF INTEREST
None
STATEMENT ON PATIENT CONSENT
The patient provided written consent for the publication of their clinical details and images. The anonymity of the patient was protected.
REFERENCES
- Soares EC, Costa FW, Pessoa RM, et al. Giant salivary calculus of the submandibular gland. Otolaryngol Head Neck Surg 2009;140:128-129. [Google Scholar] [PubMed] [Crossref]
- Huoh KC, Eisele DW. Etiologic factors in sialolithiasis. Otolaryngol Head Neck Surg 2011;145(6):935-939. [Google Scholar] [PubMed] [Crossref]
- Mbalaso OC, Nwogbo AC, Uyanwanne NS. Huge submandibular gland calculus in Port Harcourt: a case report. The Nigerian Health Journal 2018;18:172-175. [Google Scholar]
- Ogle O. Salivary gland diseases. Dent Clin N Am. 2020;64(1):87-104. [Google Scholar] [PubMed] [Crossref]
- Koch M, Mantsopoulos K, Muller S, Sievert M, Iro H. Treatment of sialolithiasis: what has changed? An update of the treatment algorithms and a review of literature. J Clin Med. 2021;11(1):231. [Google Scholar] [PubMed] [Crossref]
- Rodrigues GHC, Carvalho VJG, Alves FA, Domaneschi C. Giant submandibular sialolith conservatively treated. Autops case reports. 2017;7(1): 9-11. [Google Scholar] [PubMed] [Crossref]
- Omokanye HK, Wuraola OA, Baba AA, Ologe FE. Physiochemical characterization of a giant submandibular gland stone in a Nigerian patient. Adv in Oral and Max Surg. 2021;3:100120. [Google Scholar] [Crossref]
- Koch M, Sievert M, Iro H, K. Mantsopoulos M, Schapher M. Ultrasound in inflammatory and obstructive salivary gland diseases: own experiences and a review of the literature. J Clin Med 2021;10(16):3547. [Google Scholar] [PubMed] [Crossref]
- Gupta A, Rattan D, Gupta R. Giant sialoliths of submandibular gland duct: report of two cases with unusual shape. Contemp Clin Dent 2103;4:78-80. [Google Scholar] [PubMed] [Crossref]
- Bisher O, Hamdy J. Surgical non aggressive approach for the delivery of 4cm salivary stone from the submnadibular salivary duct: Avoiding salivary gland removal- A case report. Int J Surg. Rep 2025;127. [Google Scholar] [PubMed] [Crossref]
- Pachisia S, Mandal G, Sahu S, Ghosh S. Submandibular sialolithiasis: a series of three case reports with review of literature. Clin Pract. 2019;9(1):1119. [Google Scholar] [PubMed] [Crossref]
- Ferneini EM. Managing sialolithiasis. J Oral Maxillofac Surg. 2021;79:1581-1582. [Google Scholar] [PubMed] [Crossref]
- Woo S.H, Kim J.P, Kim J.S, Jeong H.S. Anatomical recovery of the duct of the submandibular gland after transoral removal of a hilar stone without sialodochoplasty: evaluation of a phase II clinical trial. Br. J. Oral Maxillofac. Surg. 2014;52(10):951–956. [Google Scholar] [PubMed] [Crossref]