
ABSTRACT
Cone beam computed tomography (CBCT), which provides more accurate three-dimensional visualization of dental and periapical structures than traditional radiography, has become a game-changing imaging technique in Endodontics. This study highlights the fundamentals of CBCT, its benefits, clinical applications, drawbacks, and potential developments in Endodontics. In addition to aiding in surgical planning and outcome evaluation, CBCT provides enhanced diagnostic capabilities for identifying complex root canal morphology, periapical lesions, root fractures, and resorptive abnormalities. Not with standing these advantages, cautious use is required due to worries about radiation exposure, expense, accessibility issues, and possible interpretation problems. Its appropriate application continues to revolve around ethical considerations, such as patient safety, informed consent, and adherence to professional guidelines. Patient safety and informed consent continue to be essential components of its proper use. Recent developments, including low-dose protocols, digital workflow compatibility, and artificial intelligence integration, further enhance its therapeutic relevance. Hence, CBCT is a paradigm change in endodontic imaging; yet, to optimize patient benefit and minimize hazards, its application should be limited, evidence-based, and guided by the ALARA principle.
Keywords: Artificial Intelligence; CBCT; Dentistry; Diagnosis; Endodontics; Treatment Planning
INTRODUCTION
Cone-beam computed tomography, or CBCT, has revolutionized dental diagnostic imaging, particularly in Endodontics. Traditional two-dimensional (2D) radiographs often fail to capture the complex anatomy of surrounding structures, periapical diseases, and root canal systems [1]. With the use of CBCT's three dimensional (3D) visualization, clinicians can evaluate minute details more confidently and accurately [2].
For Endodontics, which focuses on diagnosing and treating conditions affecting the dental pulp and periapical tissues, precise imaging is crucial for successful outcomes. The ability to identify missing canals, assess resorption deficiencies, diagnose root fractures, and plan surgeries has greatly improved with CBCT. Its high-resolution volumetric data enable better patient selection, treatment planning, and post-operative assessment [3]. The ability of CBCT to overcome the limitations of traditional radiography underscores its importance in Endodontics [4].
For example, in 2D images, overlapping anatomical structures can obscure pathology or lead to incorrect diagnoses. By eliminating this superimposition, CBCT provides cross-sectional views that reveal complex or hidden anatomy [5]. This is especially beneficial for teeth with multiple roots, calcified canals, or unusual root morphology. Furthermore, in retreatment cases where previous therapies have failed and detailed anatomical information is vital, CBCT has become a crucial tool [6]. It helps detect procedural errors such as ledges, detached instruments, or perforations. By accurately locating lesions and key structures like the mandibular canal or maxillary sinus, CBCT reduces complications and enhances surgical precision in endodontic procedures.
Despite of various advantages, CBCT should be used judiciously. Careful case selection is necessary due to concerns about radiation exposure, cost, and ethical considerations. Professional organizations such as the European Society of Endodontology (ESE) and the American Association of Endodontists (AAE) emphasize the importance of using CBCT only when conventional imaging is insufficient [7]. CBCT is now considered a gold standard in complex endodontic cases and is increasingly integrated into routine practice.
LITERATURE REVIEW
Fundamentals of CBCT
Cone-beam computed tomography (CBCT) is a state-of-the-art imaging technique that creates finely detailed three-dimensional images of internal structures, facial and dental diagnostics. Clinicians can observe complex anatomical areas more clearly and accurately with CBCT [8]. The cone-shaped X-ray beam rotates around the patient’s head. The X-Ray source and detector rotate around the patient's head typically through 180° to 360°. The patient's head stays still. 2D images are taken from multiple directions and these images are reconstructed by a computer digitally into a 3D volumetric image. The final image can be viewed in axial, coronal, sagittal and cross-sectional planes [9].
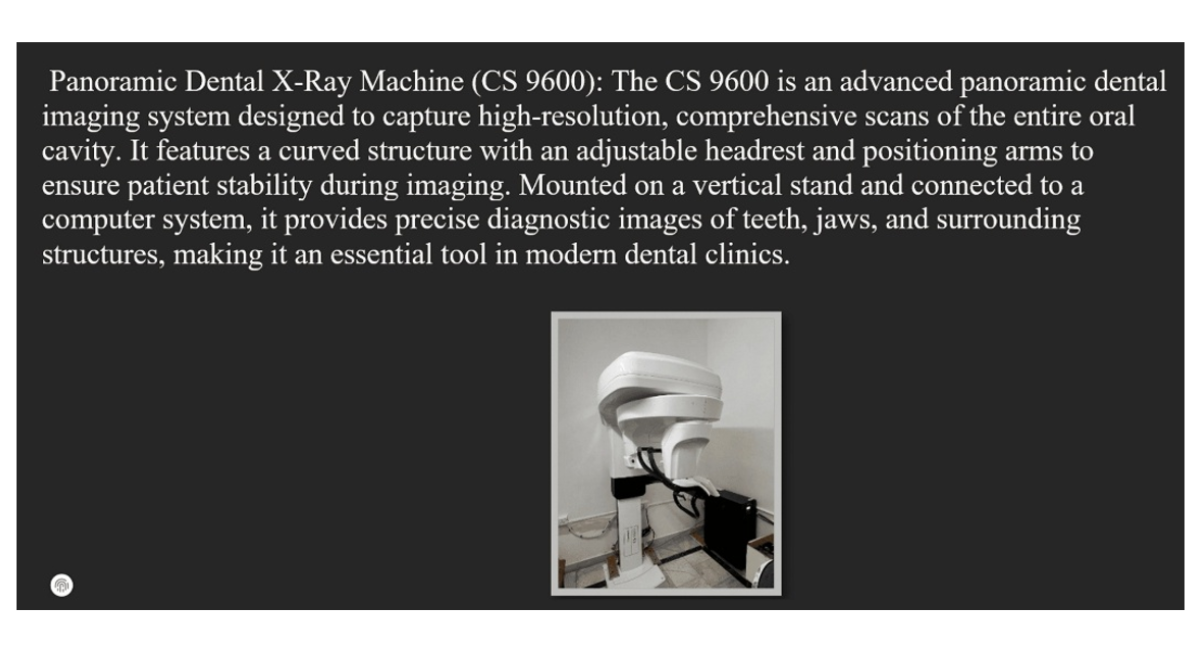
Figure 1: Dental X-Ray Machine (CS9600)
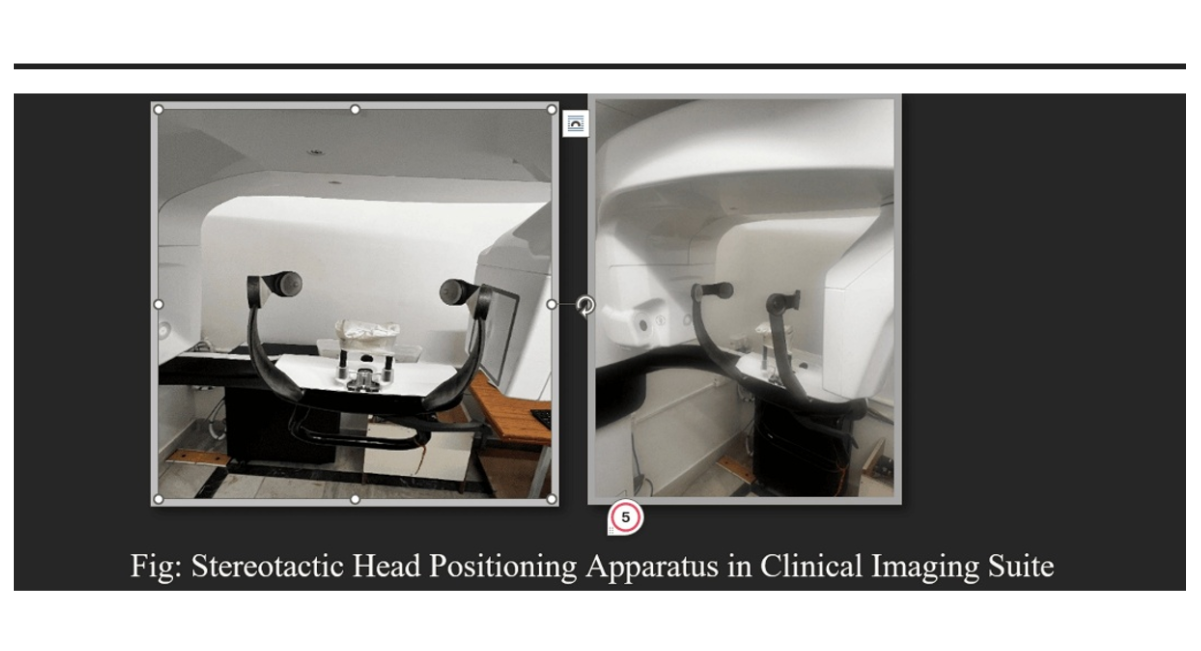
Figure 2: Stereotactic Head Positioning
The computer system uses methods such as Feldkamp-Davis-Kress (FDK) or filtered back projection to process and recreate the 3D image [10]. Obtaining and reconstructing images involves voxel-based imaging, where high-resolution images are produced using isotropic voxels, which have equal diameters in all directions [11]. The Field of View (FOV) feature enables clinicians to focus on specific areas, such as a single tooth or the entire jaw. Scan time usually falls between 10 and 40 seconds, and the radiation dose is higher than that of routine dental radiography but lower than that of conventional CT.
Aspects of image quality include spatial resolution, which is a key factor in root canal anatomy and establishes the capacity to discern minute structures. Contrast resolution refers to the capacity to distinguish between tissues with comparable densities [12]. Artifacts, which can be caused by patient movement or metal restorations, may impair image clarity.
|
Feature |
CBCT |
Conventional CT |
|
Beam shape |
Cone-shaped |
Fan-shaped |
|
Radiation dose |
Lower |
Higher |
|
Image acquisition |
Single rotation |
Multiple slices |
|
Cost and accessibility |
More affordable, dental-specific |
Expensive, hospital-based |
|
Resolution for dental structures |
High |
Moderate |
Table 1: Comparison states between CBCT and conventional CT [13]
Advantages of CBCT in Endodontics
Cone-beam computed tomography (CBCT), which enables three-dimensional (3D) visualization of teeth and adjacent tissues, has revolutionized endodontic imaging. CBCT offers several distinct advantages over traditional two-dimensional radiographs, enhancing clinical outcomes, treatment planning, and diagnostic accuracy [14]. Improved root canal anatomy visualization identifies intricate canal patterns, such as Cshaped canals, supplementary canals, and additional roots. It detects anomalous morphology and calcified canals that periapical radiography could overlook and offers cross-sectional images to help pinpoint the location of canals. Periapical pathology detection that is accurate includes greater sensitivity in detecting granulomas, cysts, and periapical abnormalities. It distinguishes between endodontic diseases and those that are not and identifies early bone alterations that 2D radiographs cannot show [15].
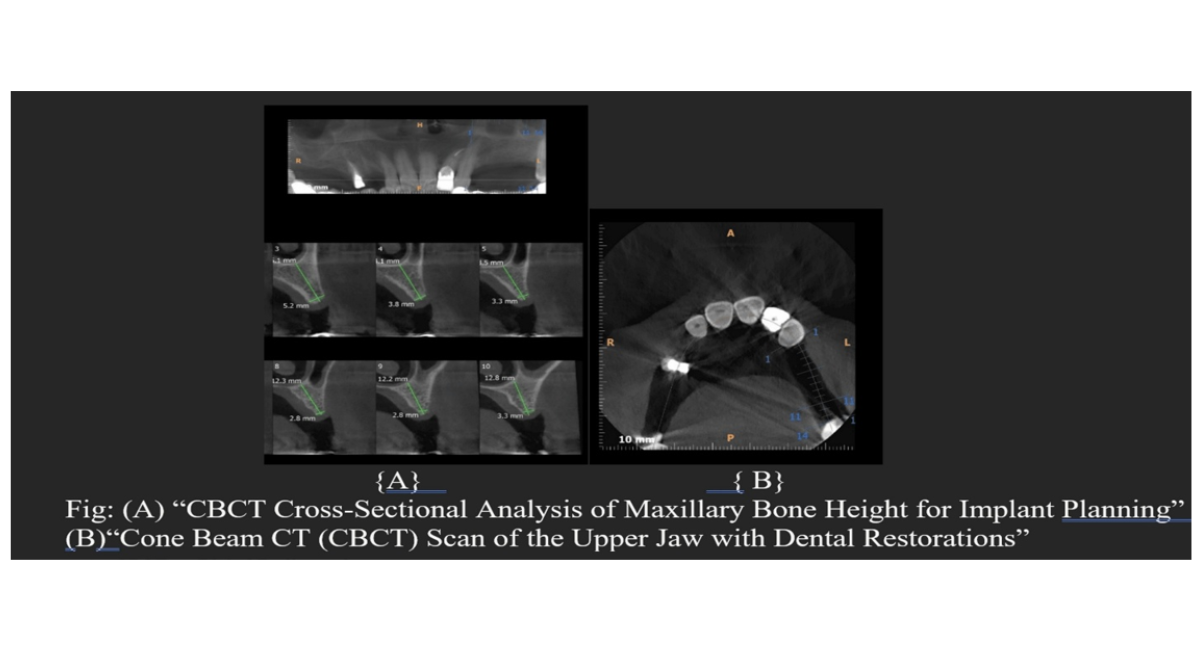
Figure 3: Applications of CBCT in Implant Planning and Post Restorative Evaluation: Axial and Cross-Sectional Views
Surgical Endodontics helps with periapical and apicoectomy planning, offers accurate lesion boundary and root apices localization, and, by mapping anatomical markers, decreases surgical risks [16]. Less distortion and superimposition remove anatomical structure overlap (e.g., roots, zygomatic arch) and offer true-tosize, undistorted photos for precise measurements. Research and education value offers top-notch photos for academic research and case documentation, and improves instruction of root canal anatomy and pathology [17].
In periapical pathology diagnosis, CBCT identifies periapical lesions before 2D radiographs do, distinguishes granulomas, cysts, and other radiolucencies, and evaluates the actual degree of bone loss in three dimensions [18].
In endodontic retreatment, CBCT identifies untreated canal or missed canals, ledges, perforations, or detached instruments, and assesses the caliber of prior obturation while pinpointing reasons for failure. For identification of resorption and root fractures, CBCT is more sensitive than periapical radiography for vertical root fractures, and both internal and external resorption can be precisely identified in terms of amount, size, and location, helping to direct the choice of treatment between extraction and restoration [19]. In endodontic surgery preoperative planning, CBCT accurately locates periapical lesions and root apices, assesses closeness to important structures such as the maxillary sinus, mental foramen, and mandibular canal, and supports the development of minimally invasive surgical techniques [20].
For assessment of therapy results, CBCT tracks the periapical lesions' recovery after therapy. Despite its advantages, CBCT has drawbacks and difficulties in Endodontics. Concerns about radiation exposure arise due to the greater radiation dose compared to normal intraoral radiography, especially in young patients and those undergoing multiple scans [21]. The ALARA (As Low As Reasonably Achievable) principle must be followed to support each exam, balancing potential risks and diagnostic benefits, and considering alternate modalities when feasible [22]. Depending on the settings and area of view, the effective dose can vary from 19 to 107 µSv. Children are particularly sensitive to radiation and require rigorous dose adjustment, while repeat scans for treatment monitoring increase lifetime exposure.
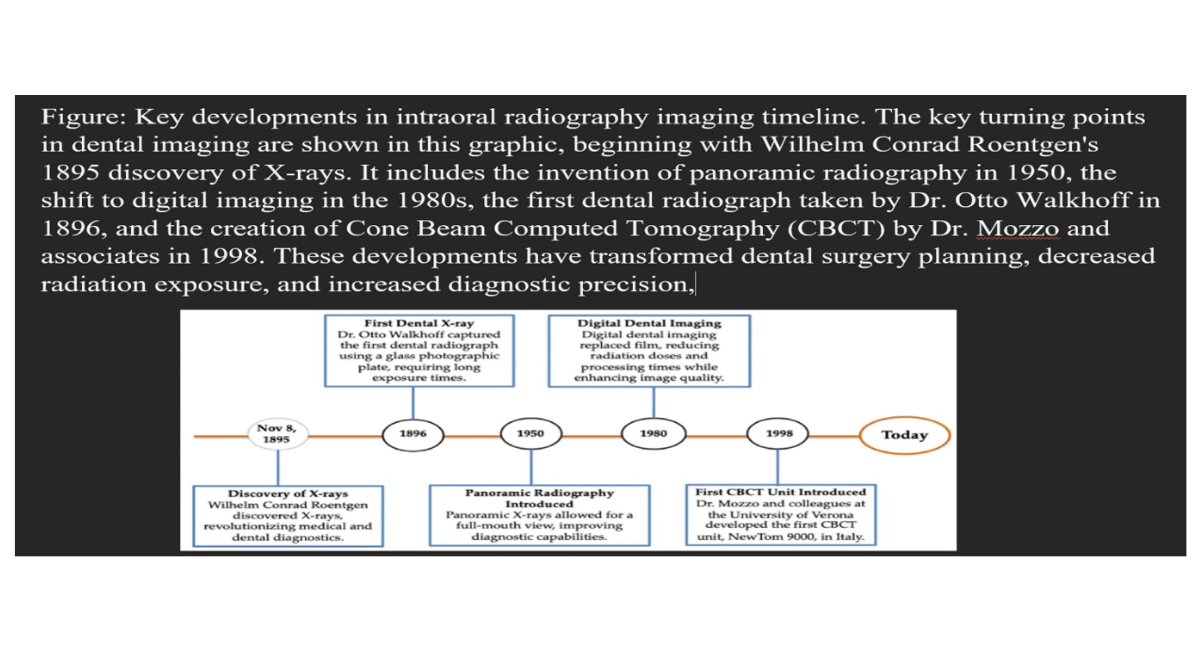
Figure 4: History of CBCT [23]
|
Feature |
CBCT |
IOPA |
|
Dimensionality |
3D volumetric imaging |
2D flate image |
|
Anatomical Detal |
Detect complex canal anatomy, additional root, periapical lesion |
Limited detail; overlapping structure may obscure pathology |
|
Radiation Dose |
Higher then IOPA |
Very low |
|
Diagnostic Accuracy |
Superior for fracture, Resorption and hidden canal |
Useful for routine diagnosis, but less sensitive |
|
Cost and Acessibility |
Expensive, less available |
Inexpensive, widely available |
Table 2: Comparison state between CBCT Vs IOPA [24]
|
Feature |
CBCT |
Digital Radiography |
|
Image Type |
3D, multi-planar |
2D, enhanced with software |
|
Resolution |
High spatial resolution (isotropic voxels) |
High resolution, but limited to 2D |
|
Radiation |
Higher dose |
Lower dose |
|
Applications |
Complex anatomy, surgical planning, resorption, fractures |
Routine diagnosis, caries detection, follow-up |
|
Interpretation |
Requires training, risk of artifacts |
Easier interpretation |
Table 3: Comparison state b/w CBCT vs Digital Radiograph [24]
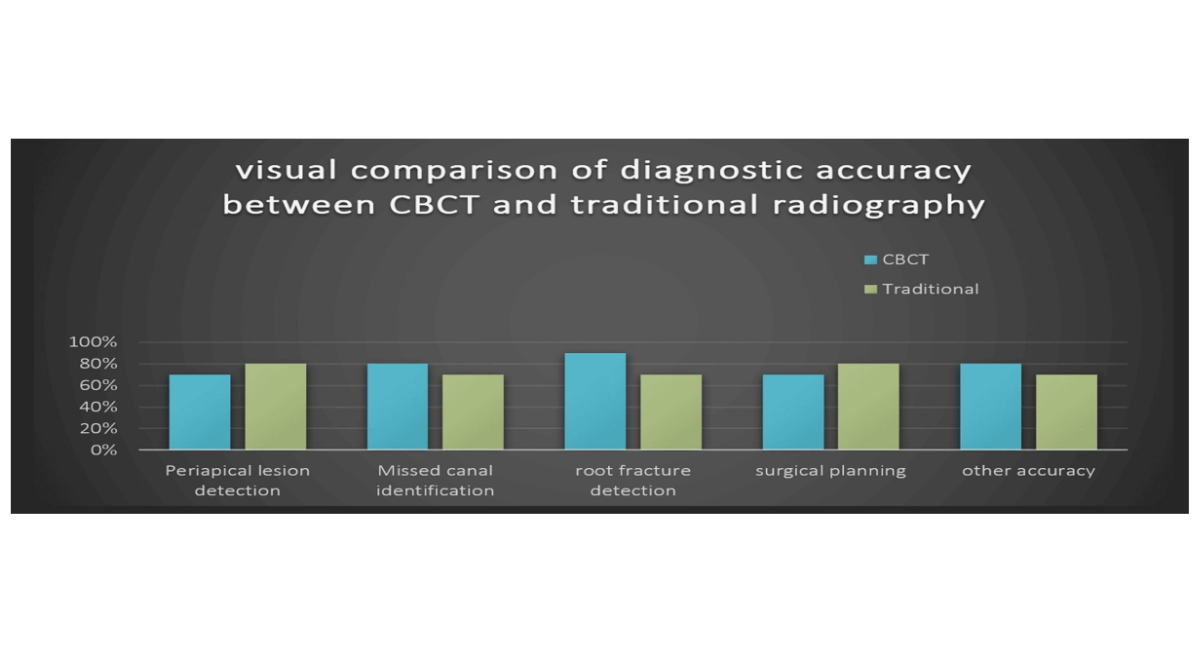
Figure 5: Visual comparison b/w CBCT and traditional radiography [25]
|
Diagnostic Task |
CBCT Accuracy (%) |
Traditional Radiography (%) |
Improvement with CBCT |
|
Periapical Lesion Detection |
85–95% |
60–70% |
+25–35% |
|
Missed Canal Identification |
80–90% |
50–60% |
+30–40% |
|
Root Fracture Detection |
90–98% |
40–60% |
40–50% |
|
Surgical Planning Accuracy |
95–98% |
60–70% |
+30–35% |
Table 4: Comparison state between CBCT and Traditional Radiography [25-26]
Applications of CBCT in Endodontics
Cone Beam Computed Tomography (CBCT) has transformed endodontic practice by providing three dimensional images of dental and periapical tissues. Unlike traditional two-dimensional radiographs, CBCT delivers volumetric data that reveals hidden root canal geometries, assesses disease severity, and guides precise treatment choices [27]. Its ability to produce multiplanar reconstructions and cross-sectional images makes it essential for both routine and complex endodontic cases. CBCT allows for complete mapping of canal systems, revealing variations such as C-shaped canals, auxiliary canals, and additional MB2 canals in maxillary molars, thereby improving canal negotiation and obturation success [28]. By acquiring volumetric data, CBCT enhances sensitivity in detecting periapical lesions, cysts, and granulomas, enabling clinicians to measure lesion size and monitor dimensional changes over time for evidence-based follow-up [29].
Standard radiographs are generally ineffective at detecting vertical and horizontal root fractures, whereas CBCT cross-sectional slices reveal fracture lines, their orientation, and extent, aiding decisions regarding preservation versus extraction. Post-treatment CBCT scans offer more accurate tracking of bone regrowth and lesion resolution than 2D imaging, contributing to therapy success, retreatment decisions, and surgical scheduling. In apicoectomy and surgical retreatment, CBCT evaluates the spatial relationship between root apices and critical anatomical landmarks such as the mandibular canal and maxillary sinus, optimizing surgical access, minimizing complications, and enhancing patient safety. CBCT also assists in managing procedural complications by locating detached instruments, ledges, and perforations within the root canal system, allowing clinicians to develop targeted retrieval or repair strategies [30]. In research and education, CBCT data support investigations into root canal morphology, disease progression, and treatment outcomes. At the same time, its integration into AR/VR platforms enriches endodontic training through immersive, interactive simulations. These diverse applications underscore CBCT’s role as a cornerstone of modern endodontic therapy, enabling clinicians to deliver more accurate, efficient, and patient-centered care when used judiciously with consideration for radiation exposure [31].
Ethical and Legal Considerations in CBCT Use
Although the use of Cone Beam Computed Tomography (CBCT) in Endodontics has greatly improved diagnostics, it also presents significant moral and legal issues for dentists [32]. While lowering hazards, responsible use guarantees that patients get the most benefit.
Guidelines for CBCT Use in Dental Practice
CBCT should only be recommended in cases where digital radiography, IOPA, or conventional imaging are insufficient for accurate diagnosis or treatment planning. Every decision to use CBCT must adhere to the ALARA (As Low As Reasonably Achievable) principle, ensuring that radiation exposure is justified and minimized. Professional standards set by organizations such as the Dental Council of India (DCI), the American Association of Endodontists (AAE), and the European Society of Endodontology (ESE) provide guidelines that practitioners must follow. To prevent misdiagnosis, CBCT scans should be interpreted exclusively by qualified medical professionals [33].
Informed Consent
Patient awareness is essential while recommending CBCT imaging. Patients should clearly understand the rationale behind the recommendation, including its advantages and disadvantages. Risks-particularly those related to radiation exposure-must be explained in simple, intelligible language. Clinicians should also inform patients about alternative imaging options, such as digital radiography and IOPA, and clarify why CBCT is the preferred choice in their specific case. Before performing the scan, voluntary written consent is required [34].
Patient Safety
Radiation protection is essential when using CBCT; clinicians should ensure the use of protective gear such as lead aprons and thyroid collars when necessary, and follow low-dose protocols, especially for children and adolescents. Data security is equally important, as CBCT images form part of the patient's official medical record and must be stored securely [35].
Research Gaps and Challenges
Clinical Validation
Multi-center studies are required to test accuracy, dependability, and safety across a range of populations, as many AI models are still in the experimental stage and lack extensive clinical trials [36].
Standardization
Currently, there are no standardized methods for integrating artificial intelligence (AI) into CBCT processes, which limits consistent implementation across clinical settings. Interoperability is further challenged by the wide variation in CBCT equipment, image formats, and software platforms, making it difficult to streamline AI applications and ensure compatibility across different systems [37].
Ethical and Legal Concerns
Clinicians must make sure that AI technologies are utilized responsibly and patients should understand their participation in treatment planning, as AI-assisted diagnosis raises concerns around responsibility and informed consent [38].
Limited Data Sets
Dental imaging lacks large annotated datasets for AI training. Most existing models train on limited, institution-specific samples, restricting generalizability [39].
Future Directions
Advancing AI integration in Endodontics requires the development of open-access CBCT datasets to support robust training of diagnostic algorithms. Incorporating real-time AI feedback during endodontic procedures can enhance clinical decision-making and improve treatment precision. To fully realize these benefits, stronger collaboration is needed between data scientists, endodontists, and radiologists to bridge the clinical and technical divide, ensuring that AI tools are both scientifically sound and practically applicable in dental practice [40].
|
USA |
Very high |
Implants, Endodontics, surgical planning |
Cost, training gaps |
Strong integration in private practices and academic centers |
|
UK |
Moderate to high |
Complex endodontic cases, trauma |
Regulatory constraints |
Emphasis on evidence-based use and radiographic justification |
|
India |
Rapidly growing |
Periapical lesions, missed canals |
Cost, access in rural areas |
Increasing use in postgraduate programs and urban clinics |
|
Germany |
High |
Root fractures, resorption, surgical planning |
Equipment standardization |
Strong academic and clinical integration |
|
Brazil |
Moderate |
Trauma, surgical planning |
Training, cost |
Expanding in urban centers with focus on continuing education |
|
China |
Rapid growth |
Orthodontics, implants |
Regulatory approval, cost |
Government support for digital dentistry expansion |
|
Middle East |
Emerging |
Implants, pathology |
Infrastructure, training |
Private sector driving adoption in UAE, Saudi Arabia |
Table 5: Global Trends in CBCT Adoption for Endodontics: A Country-by-Country Analysis [41]
Emerging Technologies in CBCT for Endodontics
Artificial Intelligence (AI)
AI algorithms are being trained to accurately recognize root canal morphology, periapical diseases, and root fractures, enhancing diagnostic precision in Endodontics. Deep learning models can automate the diagnostic process, reducing human error and saving valuable clinical time. Additionally, AI improves the clarity of CBCT images, especially in cases with low resolution or significant artifacts, thereby supporting more reliable interpretation and treatment planning [42]
Image Super-Resolution
Augmented Reality (AR) &Virtual Reality (VR)
AR and VR are being integrated with CBCT data for interactive surgical planning and dental education [43].
These tools allow clinicians and students to simulate procedures and explore 3D anatomy in immersive environments.
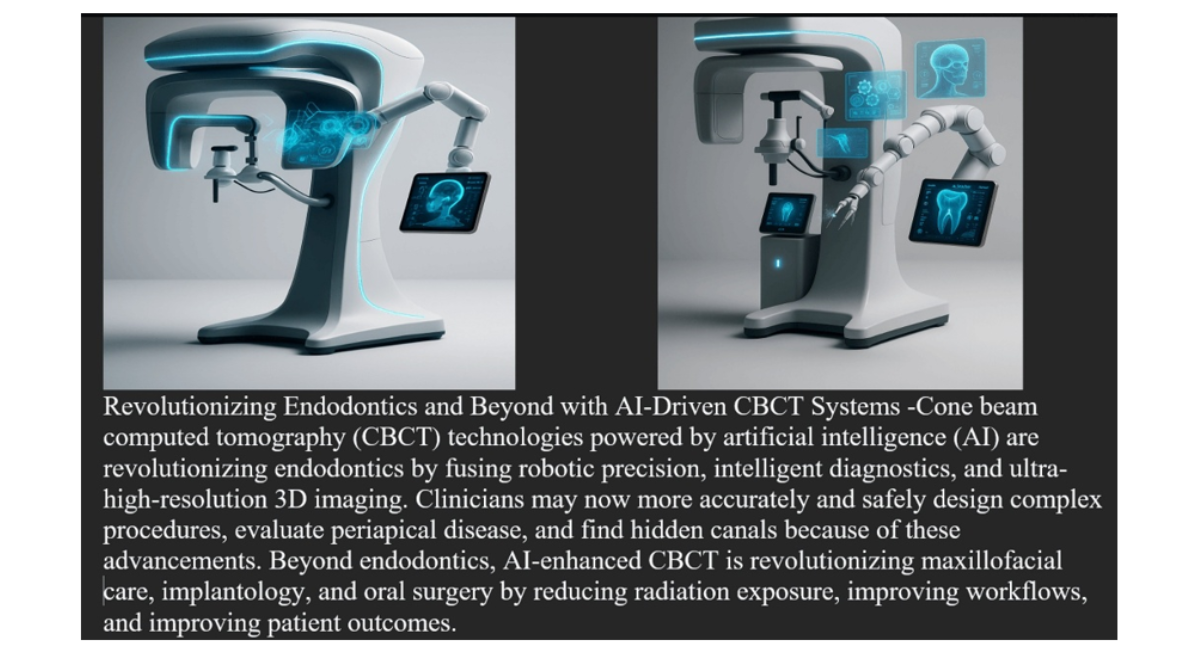
Figure 6: Next-Gen Endodontics: Robotic CBCT Systems in Action [44]
Future Trends
Emerging innovations in CBCT technology are reshaping the future of Endodontics. Personalized endodontic care is becoming possible by integrating CBCT data with genetic and systemic health information, enabling predictive modeling of treatment outcomes [45]. The development of 4D imaging, or time-based CBCT, allows dynamic visualization of anatomical changes over time, which is particularly useful for monitoring disease progression and healing [46]. Chairside and ultra-compact CBCT units are being designed for in-office use, enhancing accessibility and enabling robotic systems to guide precise access cavity preparation and endodontic microsurgery [47]. Advances in image processing software now reduce artifacts, especially those caused by metallic restorations, and improve contrast resolution for better visualization of soft tissues. Robotics integration further standardizes complex procedures, with CBCT-guided robotic systems enhancing surgical accuracy [48]. In regenerative dentistry, CBCT plays a vital role in tracking scaffold integration and tissue regeneration during pulp revascularization, offering superior insight compared to other endodontic imaging modalities [49].
CONCLUSION
Cone beam computed tomography (CBCT), which provides unmatched three-dimensional visualization of dental and periapical structures, has become a game-changing imaging technique in Endodontics. Its capacity to overcome the drawbacks of traditional two-dimensional radiography has greatly improved outcome evaluation, treatment planning, and diagnostic precision.
Clinicians can more accurately identify periapical lesions, root fractures, missing canals, and complex root canal anatomy thanks to CBCT. In surgical planning, post-operative evaluation, and retreatment instances, it is essential for bettering patient outcomes and lowering procedural complications. However, evidencebased procedures and ethical considerations-particularly those of radiation exposure and cost effectiveness-must direct the incorporation of CBCT into standard endodontic treatment.
The use of CBCT in Endodontics is expected to increase due to emerging technologies like augmented reality, artificial intelligence, and image super-resolution. Real-time feedback, improved diagnostic help, and engaging learning opportunities are all promised by these innovations. However, there are still unanswered questions about the clinical validation, standardization, and moral application of these instruments.
ACKNOWLEDGEMENT
I extend my sincere gratitude to my mentors and colleagues who have shaped my understanding of Endodontics and advanced imaging. Special thanks to Dr. Hitesh Gupta, Professor of Endodontics at Himachal Institute of Dental Sciences, Paonta Sahib, for invaluable guidance on CBCT applications and critical review of the manuscript. I am deeply appreciative of the support from the Department of Conservative Dentistry and Endodontics at Himachal Institute Of Dental Sciences, particularly Dr. Hitesh Gupta and Dr. Harshit kumar , for insightful discussions on revolutionary diagnostic tools like CBCT.
This work was supported by Dr.Harshit kumar and Dr. Hitesh Gupta (prof.dept. of conservative dentistry and Endodontics, Himachal Institute Of Dental Sciences). I also thank the librarians at library of Himachal Institute of Dental Sciences and Scopus and pubmed for facilitating access to key literature.
Finally, heartfelt thanks to my family and friends for their unwavering encouragement during the preparation of this review.
REFERENCES
- Steffen T, Winklhofer S, Starz F, Wiedemeier D, Ahmadli U, et al. Three-dimensional perception of cinematic rendering versus conventional volume rendering using CT and CBCT data of the facial skeleton. Ann Anat. 2022;241:151905. [Google Scholar] [PubMed] [Crossref]
- Li C, Teixeira H, Tanna N, Zheng Z, Chen SH, et al. The reliability of two-and three-dimensional cephalometric measurements: A CBCT study. Diagnostics (Basel). 2021;11(12):2292. [Google Scholar] [PubMed] [Crossref]
- Alhammami, Qaed Salem, Rayan Murdhi Ali Alzahrani. The Use of 3D Imaging Techniques for Improved Urological Surgical Outcomes. Metall. Mater. Eng. 2024; 30:459-69.
- Khanna AB. Applications of cone beam computed tomography in endodontics. Evid. Based Endod. 2020;5(1):1. [Google Scholar] [Crossref]
- Kadkhodayan S, Almeida FT, Lai H, Pacheco-Pereira C. Uncovering the hidden: a study on incidental findings on CBCT scans leading to external referrals. Int Dent J. 2024;74(4):808-15. [Google Scholar] [PubMed] [Crossref]
- Bhuva B, Barnes JJ, Patel S. The use of limited cone beam computed tomography in the diagnosis and management of a case of perforating internal root resorption. Int Endod J. 2011;44(8):777-86. [Google Scholar] [PubMed] [Crossref]
- Rashid M, Sharma M. AI‐assisted diagnosis and treatment planning—A discussion of how AI can assist healthcare professionals in making more accurate diagnoses and treatment plans for diseases. AI in disease detection: Advancements and applications. 2025:313-36. [Google Scholar] [Crossref]
- Jacobs R, Salmon B, Codari M, Hassan B, Bornstein MM. Cone beam computed tomography in implant dentistry: recommendations for clinical use. BMC Oral Health. 2018;18(1):88. [Google Scholar] [PubMed] [Crossref]
- Ryan S, McNicholas M, Eustace SJ. Anatomy for diagnostic imaging E-book: anatomy for diagnostic imaging E-book. Elsevier Health Sci.2024. [Google Scholar]
- Scatter correction of 4D cone beam computed tomography images for respiratory phase-dependent proton dose calculation. Diss. lmu. 2023. [Google Scholar]
- Goto M, Abe O, Hagiwara A, Fujita S, Kamagata K, et al. Advantages of using both voxel-and surface-based morphometry in cortical morphology analysis: a review of various applications. Magn Reson Med Sci. 2022;21(1):41-57. [Google Scholar] [PubMed] [Crossref]
- Versiani MA, Martins JN, Ordinola‐Zapata R. Anatomical complexities affecting root canal preparation: a narrative review. Aust Dent J. 2023;68:S5-23. [Google Scholar] [PubMed] [Crossref]
- Hajeer MY, Al-Homsi HK, Alfailany DA, Murad RM. Evaluation of the diagnostic accuracy of CBCT-based interpretations of maxillary impacted canines compared to those of conventional radiography: an in vitro study. Int Orthod. 2022;20(2):100639. [Google Scholar] [PubMed] [Crossref]
- Versiani MA, Martins JN, Ordinola‐Zapata R. Anatomical complexities affecting root canal preparation: a narrative review. Aust Dent J. 2023;68:S5-23. [Google Scholar] [PubMed] [Crossref]
- Gröndahl HG, Huumonen S. Radiographic manifestations of periapical inflammatory lesions: how new radiological techniques may improve endodontic diagnosis and treatment planning. Endodontic topics. 2004;8(1):55-67. [Google Scholar]
- Setzer FC, Kratchman SI. Present status and future directions: Surgical endodontics. Int Endod J. 2022 Oct;55:1020-58. [Google Scholar] [PubMed] [Crossref]
- Robinson DS. Modern Dental Assisting-E-Book: Modern Dental Assisting-E-Book. Elsevier Health Sciences; 2023 Apr 12. [Google Scholar]
- Cotti E, Schirru E. Present status and future directions: Imaging techniques for the detection of periapical lesions. Int Endod J. 2022;55:1085-99. [Google Scholar] [PubMed] [Crossref]
- Duyan, H. A. Z. A. L., and B. U. R. C. U: Evlice. "Evaluation of Airway Volume by CBCT in Patients with Class I and Class II Skeletal Patterns: A Pilot Study. [Google Scholar] [PubMed] [Crossref]
- Setzer FC, Kratchman SI. Present status and future directions: Surgical endodontics. Int Endod J. 2022;55:1020-58. [Google Scholar] [PubMed] [Crossref]
- Schüler IM, Hennig CL, Buschek R, Scherbaum R, Jacobs C, et al. Radiation exposure and frequency of dental, bitewing and occlusal radiographs in children and adolescents. J Pers Med. 2023;13(4):692. [Google Scholar] [PubMed] [Crossref]
- Oakley PA, Harrison DE. Death of the ALARA radiation protection principle as used in the medical sector. Dose Response. 2020;18(2):1559325820921641. [Google Scholar] [PubMed] [Crossref]
- Horner K, O'Malley L, Taylor K, Glenny AM. Guidelines for clinical use of CBCT: a review. Dentomaxillofac Radiol. 2015;44(1):20140225. [Google Scholar] [PubMed] [Crossref]
- Roy CA. Comparison of Accuracy and Reliability of Cone Beam Computed Tomography Versus Intraoral Periapical Radiography for Detecting Simulated External Root Resorption (Master's thesis, Rajiv Gandhi University of Health Sciences (India)). [Google Scholar] [Crossref]
- Sherrard JF, Rossouw PE, Benson BW, Carrillo R, Buschang PH. Accuracy and reliability of tooth and root lengths measured on cone-beam computed tomographs. Am J Orthod Dentofacial Orthop. 2010;137(4):S100-8. [Google Scholar] [PubMed] [Crossref]
- Xu W, An G, Yu J, Zhang Y, Zhao X, et al. Accelerated Monte Carlo-driven statistical reconstruction for CBCT scatter correction. Opt Express. 2025;33(8):18264-90. [Google Scholar] [PubMed] [Crossref]
- Bhatt A, Grover S, Khanna M. CAPTURING THE FUTURE OF DENTISTRY: A JOURNEY THROUGH DIGITAL IMAGING. DENTOMED PUBLICATION HOUSE; 2025. [Google Scholar]
- Li S, Min Z, Wang T, Hou B, Su Z, et al. Prevalence and root canal morphology of taurodontism analyzed by cone-beam computed tomography in Northern China. BMC Oral Health. 2025;25(1):5. [Google Scholar] [PubMed] [Crossref]
- Mackiewicz E, Bonsmann T, Kaczor-Wiankowska K, Nowicka A. Volumetric assessment of apical periodontitis using cone-beam computed tomography—A systematic review. Int J Environ Res Public Health. 2023;20(4):2940. [Google Scholar] [PubMed] [Crossref]
- Fan Y, Gao Y, Wang X, Fan B, Chen Z, et al. Expert consensus on management of instrument separation in root canal therapy. Int J Oral Sci. 2025;17(1):46. [Google Scholar] [PubMed] [Crossref]
- de Magalhães AA, Santos AT. Advancements in diagnostic methods and imaging technologies in dentistry: A literature review of emerging approaches. J Clin Med.. 2025;14(4):1277. [Google Scholar] [Crossref]
- Jain PR, De Lemos AN. Legal Considerations in Endodontics. InCommon Complications in Endodontics: Prevention and Management. 2025;(pp. 321-349). [Google Scholar] [Crossref]
- Mota de Almeida FJ, Knutsson K, Flygare L. The effect of cone beam CT (CBCT) on therapeutic decision-making in endodontics. Dentomaxillofac Radiol. 2014;43(4):20130137. [Google Scholar] [PubMed] [Crossref]
- Hartshorne J. Essential guidelines for using cone beam computed tomography (Cbct) in dentistry. Radiation dose, risks, safety, ethical and medico-legal considerations. Int Dent Afr Ed.. 2022;12(5):26-33. [Google Scholar]
- Krishna UV, Addepalli L, SD VS, Jaime LM. Enhancing Airway Assessment with a Secure Hybrid Network-Blockchain System for CT & CBCT Image Evaluation. Int Res J Multidiscip Technov. 2024;6(2):51-69. [Google Scholar] [Crossref]
- Das MK. Multicenter studies: relevance, design and implementation. Indian Pediatr. 2022;59(7):571-9. [Google Scholar] [PubMed] [Crossref]
- Rashid M, Sharma M. AI‐assisted diagnosis and treatment planning—A discussion of how AI can assist healthcare professionals in making more accurate diagnoses and treatment plans for diseases. AI in disease detection: Advancements and applications. 2025 Jan 8:313-36. [Google Scholar] [Crossref]
- Khalifah AM, Alafaleg R. Artificial Intelligence in Dental Education: A Scoping Review of Opportunities, Challenges, and Ethical Frameworks for Shaping Accreditation Standards and Future Practice. [Google Scholar] [Crossref]
- Ali MA. The Role of Artificial Intelligence in Modern Dentistry: Applications, Challenges, and Future Directions. Future Dental Research. 2024;2(2):39-49. [Google Scholar] [Crossref]
- Rahim A, Khatoon R, Khan TA, Syed K, Khan I, et al. Artificial intelligence-powered dentistry: Probing the potential, challenges, and ethicality of artificial intelligence in dentistry. Digital health. 2024;10:20552076241291345. [Google Scholar] [PubMed] [Crossref]
- Rigo DC, de Oliveira Rocha A, Dos Anjos LM, Santos PS, Ramos I, et al. A global overview of the use of cone beam computed tomography in dentistry: a bibliometric review focusing on paediatric patients. F1000Res. 2025;13:1320. [Google Scholar] [PubMed] [Crossref]
- Ji Y, Chen Y, Liu G, Long Z, Gao Y, et al. Construction and evaluation of an AI-based CBCT resolution optimization technique for extracted teeth. . 2024 Sep 1;50(9):1298-306. [Google Scholar] [PubMed] [Crossref]
- Lin PY, Chen TC, Lin CJ, Huang CC, Tsai YH, et al. The use of augmented reality (AR) and virtual reality (VR) in dental surgery education and practice: A narrative review. J Dent Sci. 2024;19:S91-101. [Google Scholar] [PubMed] [Crossref]
- Xue X, Ding Y, Shi J, Hao X, Li X, et al. Cone beam CT (CBCT) based synthetic CT generation using deep learning methods for dose calculation of nasopharyngeal carcinoma radiotherapy. Technol Cancer Res Treat. 2021;20:15330338211062415. [Google Scholar] [PubMed] [Crossref]
- Patil SR, Karobari MI. Exploring artificial intelligence for enhanced endodontic practice: Applications, Challenges, and future directions. Adv Public Health. 2024;2024(1):8075515. [Google Scholar] [Crossref]
- Borse K, Shende P. 3D-to-4D structures: an exploration in biomedical applications. AAPS PharmSciTech. 2023;24(6):163. [Google Scholar] [PubMed] [Crossref]
- Elmatary A, Moawad E, Heidarifar O, Stone S. Endodontic access cavity preparation: challenges and recent advancements. Br Dent J. 2025;238(7):469-75. [Google Scholar] [PubMed] [Crossref]
- Chahla B, Ozen M. Fluoroscopy and Cone Beam CT Guidance in Robotic Interventions. Techniques in Vascular and Interventional Radiology. 2024;27(4):101007. [Google Scholar] [PubMed] [Crossref]
- Alsuraifi A, Ayad R, Mohammed NA, Al-Essa UI, Mohammed Z, et al. Endodontics at the Bio-Futuristic Frontier: Integrating High-Resolution Imaging, Regenerative Therapies, and Nanotechnology for Next-Generation Care. [Google Scholar] [Crossref]